
Why Age 7? The Golden Window for an Orthodontic Check-Up
By age seven, most children possess a unique mix of primary (baby) teeth and permanent (adult) teeth. This “mixed dentition” stage is vital because the first permanent molars have typically erupted, establishing the “back bite.”
An evaluation at this age allows Dr. Bob Kumra or Dr. Mina Abdolahi to assess front-to-back and side-to-side tooth relationships. While many seven-year-olds will not require immediate braces, this screening allows us to:
- Identify Jaw Growth Issues: We can spot subtle problems with jaw symmetry while the bone is still malleable.
- Monitor Eruption Paths: We ensure permanent teeth have a clear path to emerge, preventing impactions.
- Assess the “Back Bite”: Establishing the relationship between the upper and lower jaw early prevents complex skeletal issues later.

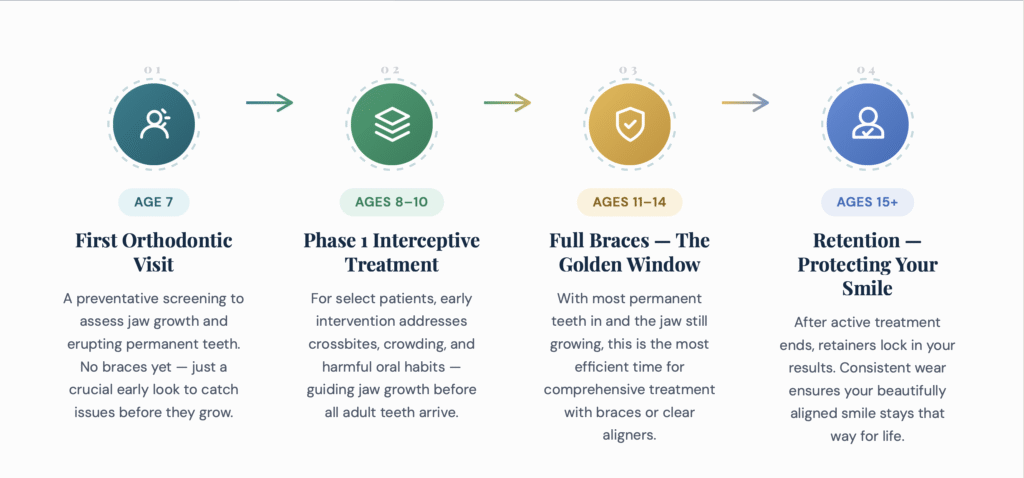
The Smile Timeline: A Visual Guide to Your Child’s Orthodontic Journey
The First Check-Up: Why Age 7 is the Magic Number
The AAO’s recommendation for a check-up by age 7 often surprises parents. The goal isn’t to put braces on a second-grader. Instead, this early evaluation is the most important step in preventative care. By this age, the first adult molars have typically erupted, establishing the back bite. This allows an orthodontist to spot subtle issues with jaw growth or emerging teeth that may become significant problems later.
Think of it as a wellness check for your child’s future smile. Early detection can simplify or even eliminate the need for more complex treatment down the road.
What We Look For in a 7-Year-Old: The 5-Point Smile Check for Parents
When you look at your child’s smile, you can watch for the same key indicators we assess during a clinical exam. Here is a simple checklist of things to look for:
- Severe Crowding or Spacing: Noticeable overlapping of teeth or large gaps where permanent teeth have come in. This happens when the jaw is too small or teeth are too large to fit correctly.
- Crossbites (Front and Back): When you look at your child’s bite, the upper teeth should sit slightly outside the lower teeth, like a lid on a box. If any bottom teeth sit outside the top teeth, it’s a crossbite. This can cause lopsided jaw growth if left unaddressed.
- Overbites (Overjet) & Underbites: An overjet is when the top front teeth protrude far forward (“buck teeth”), making them prone to injury. A deep overbite is when the top teeth cover too much of the bottom teeth.
- Harmful Oral Habits: Persistent thumb or finger sucking past age 5 can physically reshape the jawbone and flare the front teeth out, often creating an “open bite” where the front teeth don’t touch.
- Jaw Growth & Symmetry: Look at your child’s chin. Does it seem shifted to one side? Do the midlines of the top and bottom teeth line up? Asymmetry can indicate a growth imbalance that is best guided at a young age.
Early (“Phase 1”) Treatment: 5 Signs Your Child Might Need Braces with Baby Teeth
Phase 1 treatment, often called interceptive orthodontics, occurs while a child still has most of their primary (baby) teeth. This period, roughly between the ages of 6 and 12, is known as the mixed dentition stage.
The goal of Phase 1 isn’t to create a “perfect” Hollywood smile; that’s what teen orthodontics are for. Instead, interceptive treatment is about stopping a problem before it fully forms. Think of it as correcting the “foundation” of the house while the walls are still being built.
The American Association of Orthodontists (AAO) recommends a child have their first evaluation by age 7. At this age, the first permanent molars have usually erupted, establishing the back bite and allowing an orthodontist to evaluate the relationship between the upper and lower jaws.
Typically, Phase 1 lasts between 9 and 12 months. Once the specific structural goal is achieved, the braces or appliances are removed, and the child enters a “rest period” (monitoring) while the remaining permanent teeth erupt. Phase 2 the comprehensive treatment most people recognize usually begins around age 11 to 13.
1. Severe Crowding or Spacing
If there is insufficient room in the jaw, incoming adult teeth may become “stuck” (impacted) or erupt in the wrong direction. Conversely, extreme spacing may indicate a mismatch between tooth size and jaw width.

2. Problematic Bites (Crossbite, Underbite, Overbite)
- Crossbite: Occurs when upper teeth bite inside the lower teeth. If left untreated, the jaw may shift to one side to compensate, leading to permanent facial asymmetry and asymmetric loading on the Temporomandibular Joints (TMJ).
- Underbite: Often characterized by mandibular prognathism (a protruding lower jaw), an underbite can restrict the forward growth of the upper jaw and lead to a concave facial profile.

3. Protruding Front Teeth (“Buck Teeth”)
Teeth that protrude significantly are at a higher risk of trauma or accidental fracture, especially in active children. Early treatment can guide these teeth back into a safer position.
4. Harmful Oral Habits
Prolonged thumb-sucking or tongue-thrusting (moving the tongue forward against the teeth during swallowing) can physically reshape the developing alveolar bone. This often results in an anterior open bite, where the front teeth do not touch even when the mouth is closed.
5. Early or Late Loss of Baby Teeth
Baby teeth act as placeholders. If a tooth is lost too early due to decay, adjacent teeth may undergo mesial drift, sliding into the empty space and blocking the permanent tooth underneath.
The Benefits of Acting Early: More Than Just a Straighter Smile
Intervening during the mixed dentition phase offers several clinical advantages:
- Guiding Jaw Growth: Using appliances like palatal expanders can widen a narrow upper arch, creating room for crowded teeth and improving facial symmetry.

- Reducing Future Extractions: By creating space now, we often avoid the need to extract permanent premolars later. Research indicates that early transverse expansion can increase non-extraction success rates from 60% to over 90%.
- Shortening Phase 2: Correcting the “heavy lifting” skeletal issues now often makes the second phase of braces much shorter and less complicated.
- Preserving “Leeway Space”: We can use space maintainers to hold the 2.5mm of “leeway space” per side in the lower jaw, allowing crowded incisors to align naturally as permanent teeth erupt.
What Comes After Phase 1 (Phase 1 vs. Phase 2 Orthodontics)
The most common question we hear is: “If I do this now, is my child finished?”
In the vast majority of cases, the answer is no. Phase 2 is still typically needed when the child is 11–13 to fine-tune the position of all the permanent teeth. However, Phase 1 makes Phase 2 significantly easier.
When we address a skeletal or eruption issue early, Phase 2 is often:
- Shorter: 12 months instead of 24.
- Simpler: No extractions of permanent teeth.
- More Stable: The foundation was built correctly, leading to a better long-term result.
Between Phase 1 and Phase 2, there is a “Rest Period.” During this time, we provide a retainer and see your child every six months to monitor their growth. We use this time to celebrate their progress and ensure their self-esteem continues to grow along with their smile.
The “Braces Years”: Why Ages 10-14 Are the Ideal Time for Treatment
This age range is considered the “golden window” for comprehensive orthodontics because it presents a perfect storm of biological advantages. Most, if not all, permanent teeth have erupted, and adolescents are typically in their pubertal growth spurt.
The Science of the Teen Smile: Growth & Timing
An orthodontist can leverage a teen’s natural growth to correct bite issues and align the jaws much more effectively. Think of it like molding clay when it’s still soft. During these years, the jawbone is more pliable and responsive to the gentle forces of braces or aligners. We can guide the teeth and jaw into their ideal positions with less effort and in less time than would be required once growth is complete. This is the most efficient and effective time for a full smile transformation.
What About Adults? Is There a “Too Old” for Braces?
We often hear adults ask, “Am I too old for braces?” The answer is a definitive no. There is no upper age limit for orthodontic treatment. In fact, adults over 50 are one of the fastest-growing demographics in our DC and Stafford clinics.
Adult orthodontics often focuses on:
- Pre-Restorative Alignment: Moving teeth to create space for future implants, bridges, or veneers.
- Periodontal Health: Aligning crowded teeth to make them easier to clean, reducing the risk of gum disease.
- Biological Considerations: While bone remodeling is slower in adults (often resulting in 20-30% longer treatment times), success rates remain high as long as the supporting bone and gums are healthy.
Beyond Aesthetics: The Health Benefits of Straightening Adult Teeth
While a beautiful smile is a primary motivator, the health benefits of adult orthodontics provide a compelling long-term return on investment.
- Preventing Gum Disease: Straight teeth are easier to clean. Crowded or misaligned teeth create havens for plaque, increasing the risk of cavities, gingivitis, and bone loss.
- Alleviating Jaw Pain (TMJ): A bad bite forces your jaw into an unnatural position, straining the joints and muscles. This can lead to chronic headaches, clicking, and pain. Correcting the bite establishes a balanced, comfortable jaw position.
- Reducing Uneven Tooth Wear: When your bite is misaligned, some teeth bear more force than others. This leads to premature chipping, fractures, and enamel erosion, often requiring crowns or other restorative work later in life.

Orthodontic Options at Kumra Ortho: Technology for Every Age
We utilize state-of-the-art technology to make treatment faster and more comfortable than ever before.
Modern Braces for Kids & Teens
We offer self-ligating braces, which use a specialized sliding door mechanism to hold the archwire. This reduces friction, allowing teeth to move more freely and comfortably. They also lack the elastic ties that often trap plaque and stain easily.
Invisalign First® for Young Patients
Designed specifically for children aged 6 to 10, Invisalign First uses SmartStage technology to expand the dental arch and create room for incoming permanent teeth. These aligners feature “eruption compensation” tabs that allow new teeth to emerge into the correct position without obstruction.
How to Evaluate Conflicting Recommendations
If you’ve received two different opinions, you aren’t alone. Many parents in the DC and Stafford corridor find themselves caught between a “let’s do everything now” approach and a “wait and see” approach. Use this checklist to evaluate your consultation:
Green Flags (Signs of a Conservative Clinician)
- Specific Diagnosis: They name a clinical condition (e.g., “Posterior Crossbite”) rather than vague “bite issues.”
- The “Wait” Explanation: They can clearly explain exactly what would change if you waited 12–18 months.
- Observation Clubs: They offer a “Growth and Guidance” program where they see your child every 6 months for free to monitor development without rushing into hardware.
- Honest Tradeoffs: They admit that Phase 1 may not eliminate the need for Phase 2, but will likely make it shorter and less complex.
Red Flags (High-Pressure Tactics)
- Vague Rationale: They use phrases like “his teeth are just really crowded” without discussing jaw structure.
- Manufactured Urgency: They claim your child “will need surgery” if you don’t start today, specifically for issues that are clearly dental rather than skeletal.
- The “One-Price” Guarantee: They imply that Phase 1 is a “guarantee” that your child will never need braces again.
- No “Wait” Option: They refuse to discuss what happens if you choose to monitor rather than treat.
Understanding the orthodontic costs in DC and Stafford is a key part of this evaluation. Phase 1 typically costs between $2,000 and $4,000. If this is recommended, it should be because it reduces the future risk of $10,000+ jaw surgeries or permanent tooth extractions.

Your Child’s First Visit: What to Expect at Your Complimentary Consultation
We believe in a “no-surprises” approach. During your complimentary consultation in Washington, DC or Stafford, you can expect:
- A Warm Welcome: Meet our multilingual team (fluent in English, Spanish, Tagalog, Hindi, and Farsi).
- Quick & Easy Digital Scans: We use the iTero Element scanner to create a high-resolution 3D map of the mouth. No goopy, gag-inducing molds are required.
- Outcome Simulator: Using iTero technology, we can show you a side-by-side comparison of your child’s current smile and their projected post-treatment result in real-time.
- A Thorough Exam: Dr. Kumra or Dr. Abdolahi will personally examine the relationship between the teeth, jaw, and facial profile.
- Transparent Pricing: We provide a clear breakdown of costs and insurance coverage. In the DMV region, Phase 1 treatment typically ranges from $2,500 to $4,800, and we offer flexible, 0% interest payment plans to fit your budget.



